
Percutaneus radiofrequency rhizotomy for the managment of severe spastic paraplegia in adults.
DOI:
https://doi.org/10.47924/neurotarget202126Keywords:
Spastic Paraplegia, Rhizotomy, Minimally Invasive SurgeryAbstract
Introduction: Severe spastic paraplegia is a comoon condition in spinal cord injury, when medical treatment fails, the most common surgical treatment is intrathecal baclofen therapy and selective dorsal rhizotomy. We propose the lesion of the root at the foraminal level by radiofrequency percutaneous rhizotomy (RF-DRG) as a minimally invasive, useful and low-cost option.
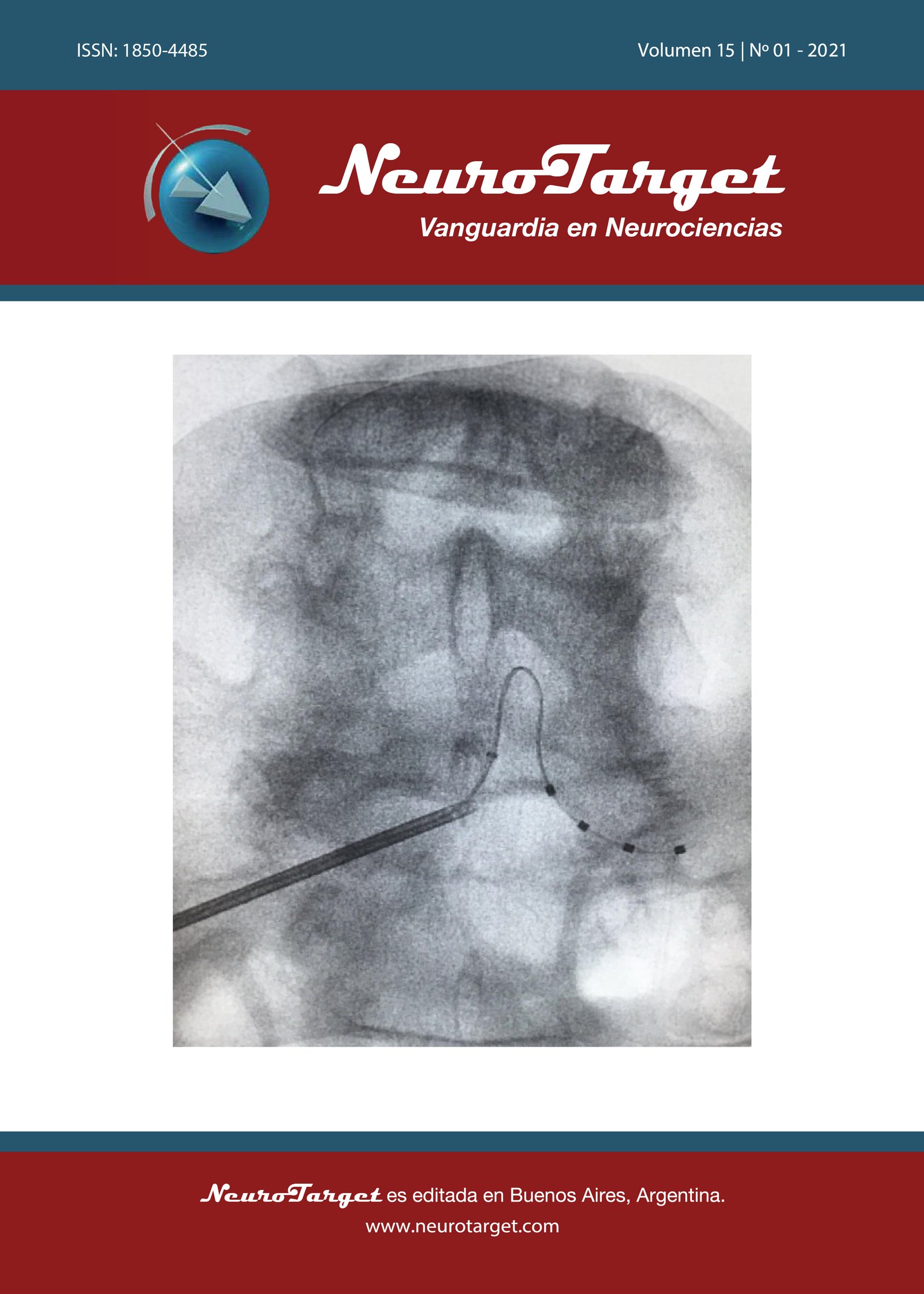
Materials and methods: The surgical technique is described in one case where foraminal RF-DRG was performed in a patien with severe flexor/adductor hip stasticity associated with severe spasms and pain that limits personal care. The patient was evaluated by a multidisciplinary team throughout its evolution using the scales of Spasm Frequency Scale (SFS), Medical Research Council Scale (MRC), Modified Asworth Scale (MAS), Adductor Tone Rating (ATRS) and Global Pain Scale (GPS).
Results: The procedure was performed once, and we found a 50% improvement in SFS, MAS, ATRS and GPS. This has enabled him to improve his quality of life with respect to personal and sexual care. The patient had a follow-up at 5 years and didn´t need to repeat RF-DRG.
Discussion: RF-DRG is proposed for severe paraplegic patients (MRC 0), with spasms, clonus and severe uncontrollable and intractable spasticity. RF-DRG is a minimally invasive and reproducible technique.
Conclusion: RF-DRG is an option for sequential paraplegic patients with severe spasticity. Its effectiveness over time should be defined with long-term controlled studies.
Metrics
References
Khurana SR, Garg DS. Spasticity and the use of intrathecal baclofen in patients with spinal cord injury. Phys Med Rehabil Clin N Am. 2014;25(3):655-ix. doi: 10.1016/j.pmr.2014.04.008
Sitthinamsuwan B, Phonwijit L, Khampalikit I, Nitising A, Nunta-aree S, Suksompong S. Comparison of efficacy between dorsal root entry zone lesioning and selective dorsal rhizotomy for spasticity of cerebral origin. Acta Neurochir (Wien). 2017 Dec;159(12): 2421-2430
Kasdon D, Lathi E. A Prospective Study of Radiofrequency Rhizotomy in the Treatment of Postraumatic Spasticity. Nerosurgery, 1984. Vol. 15, N°4: 526-529
Herz D et al. The Management of Paralytic Spasticity. Neurosurgery, 1990. Vol. 26, N°2: 300-306
Herz D, Parsons K, Pearl L. Percutaneous Radiofrequency Foramenal Rhizotomies. Spine, 1893. Vol 8, N°7: 729-732
Kasdon D. Controversies in the Surgical Manegement of Spasticity. Clin Neursurg. 1896; 33:523-529
Penn RD. lntrathecal haclofen for severe spasricity. Ann N Y Acad Sci 1988; 53 I: I S766.
Medical Research Council. Aids to the examination of the peripheral nervous system, Memorandum no. 45, Her Majesty’s Stationery Office, London, 1981.
Bohannon RW, Smith MB: Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys Ther 1987, 67(2):206207
Snow BJ, Tsui JK, Bhatt MH, Varelas M, Hashimoto SA, Calne DB. Treatment of spasticity with botulinum toxin: a double-blind study. Ann Neurol 1990; 28: 512–515
Gentile DA, Woodhouse J, Lynch P, Maier J, McJunkin T. Reliability and validity of the Global Pain Scale with chronic pain sufferers. Pain Physician. 2011;14(1):61-70.
Lance JW. What is Spasticity? The Lancet 1980; 335: 606.
Silva, C., 2013. Semiología Y Fundamentos De La Neurología Clínica. 1st ed. Santiago: AMOLCA, pp.64-65.
Bolaños Jiménez R, et al. Espasticidad, conceptos fisiológicos y fisiopatológicos aplicados a la clínica. Rev Mex Neuroci 2011; 12(3): 141 148
Bellofatto M, De Michele G, Iovino A, Filla A and Santorelli FM (2019) Management of Hereditary Spastic Paraplegia: A Systematic Review of the Literature. Front. Neurol. 10:3. doi: 10.3389/fneur.2019.00003
Vles G, et al. Percutaneous radiofrequency lesions adjacent to the dorsal root ganglion alleviate spasticity and pain in children with cerebral palsy: pilot study in 17 patients. BMC Neurology 2010, 10:52
Farmer JP, Sabbagh AJ: Selective dorsal rhizotomies in the treatment of spasticity related to cerebral palsy. Childs Nerv Syst 2007, 23(9):991-1002.
Langerak NG, Lamberts RP, Fieggen AG, Peter JC, van der Merwe L, Peacock WJ, Vaughan CL: A prospective gait analysis study in patients with diplegic cerebral palsy 20 years after selective dorsal rhizotomy. J Neurosurg Pediatr 2008, 1(3):180-186.
Martínez I, Abad J, 2015. Parálisis Cerebral Infantil. Manejo de las alteraciones musculoesqueléticas asociadas. 1st ed. Madrid: Ergon, pp.41-50.
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2021 Marcos Baabor Aqueveque, Hernán Delso Páez, Bayron Valenzuela Cecchi

This work is licensed under a Creative Commons Attribution 4.0 International License.
The article is distributed under the Creative Commons Attribution 4.0 License. Unless otherwise stated, associated published material is distributed under the same licence.





